
February 2, 2022
I (Sam) am far from alone in wondering how different societies on the globe will approach masking norms and regulations for the prevention of respiratory viruses years from now. Part of the reason I chose to write about the near-term future of masking in this newsletter is that I’m not entirely sure what my (and my family’s) own personal masking choices will or should be in every social circumstance.
Masking during the COVID pandemic:
For the bulk of the pandemic I have been solidly in favor of mask mandates for indoor public settings. Here in our team room, there was that short but liberating window when we unmasked after we were all fully vaccinated but before the Delta variant arrived. More recently, as the highly infectious Omicron variant is rapidly overtaking Delta, the importance for masking among vaccinated people has come to include flattening the curve of healthcare and other essential worker absenteeism, in addition to preventing illness.
Looking back, it is fair to say that the public health messaging around masking has been a bit herky jerky, mostly justified by lack of knowledge at the time. Remember when the worry about contacting covid from touching surfaces (and then touching your mouth/nose) seemed as big or bigger in the press than the worry about respiratory droplets? I do, in part owing to that early New England Journal of Medicine article showing intact virus on plastics and stainless steel for up to 72 hours after inoculation. That article was later de-emphasized because the inoculums used in those experiments were exponentially larger than what was suspected to be contained within a respired/coughed/laughed droplet of a covid-infected human and the decay in the virus titre across on all experimental surfaces was predictably exponential.
Then there were the healthcare worker colleagues of mine working in hospitals who received verbal wrist slaps for wearing a mask in locations outside of the ER or ICU. That messaging, and similar parallel messaging to the public that they didn’t need to rely on masking to prevent covid, seemed to fall under the category of saving the masks for the most exposed healthcare workers (reasonable!) but wasn’t always voiced clearly as such.
Then there was the lengthy debate about whether a mask was better at preventing the infected person from spreading infection or the uninfected person from getting infected. The important answer, with caveats on the type of mask used, is both, but as I recall, most of the early public health messaging emphasized protection of spreading to others. Once it became clear that well-masked healthcare workers who avoided eating in the breakrooms didn’t seem to have higher rates of infection than non-healthcare workers, the messaging about protecting yourself with a mask began to grow louder.
I remain proud to live in a state that errs on the side of public health caution. Even when the science never supported an appreciable covid transmission risk from casual uncrowded contact in outdoor settings, I pulled my mask up over my face when jogging or walking past someone else who was wearing their mask, as if to salute their level of care and intention. I’m unable to do that now though, by the way, as I no longer wear a mask around my neck while jogging, if at all outside.
Masking during endemic SARS-CoV-2 virus:
All that is about masking during the covid pandemic, though. What about masking during the upcoming predicted scenario of an endemic SARS-CoV-2 virus, after this current massive Omicron wave, however long it lasts, finishes adding its numbers to the group of people with partial immunity from vaccine, infection, or both? An endemic SARS-CoV-2 virus is one that is always present at some level in the population but is relatively (not completely) consistent and predictable in rate or pattern. The hope and probability is that through vaccines, periodic re-infection, and a range of treatment options to prevent high risk people from dying, endemic SARS-CoV-2 gets relegated to an inferior rank of threatening pathogen, even as new variants keep coming. Many newspaper articles tell us that the scientific community is converging on this probability, even if the finer predictions of its timing remain debated.
Disease-predicting researchers at the Institute for Health Metrics and Evaluation (IHME) here at UW are as well-suited as any to predict endemic SARS-CoV-2. During a January 21st presentation, IHME’s Director, Chris Murray, has this to say:
“We will go into this period where the immunological exposure to COVID is so much higher, both from vaccination and infection, that we won’t see restrictions return, so I think we will go back to normal in the sense that we won’t have major restrictions on behavior.” … “From an individual standpoint, personally, I’m going to be cautious until the wave is through, which is just a few weeks away. Once the wave is through, I think everybody will have to make their own choice,” said Murray.
This past weekend in the Seattle Times, columnist Danny Westneat wrote a piece titled, “A UW expert just called the end of the pandemic. Why is nobody celebrating?” In it, he wondered what might be behind the lack of public celebration: Once bitten twice shy?…Timeline is too confident?… Believe it when I see it?… I’m already done with covid?… Don’t say that while the hospitals are slammed?
I’ve already confessed to you that I’m an Omicron optimist. I wouldn’t wish covid upon anyone but feel pretty lucky for the global population that the SARS-CoV-2 variant that happens to be infectious enough (incredibly infectious) to be succeeding in displacing the Delta variant and filling in much of the residual pocket of zero-immunity (ie, unvaccinated people with no past infection) is significantly less virulent than Delta (notice I didn’t call it mild). In the latest example of that, Kaiser Permanente in Southern California recently wrote up (not yet peer-reviewed) a comparison of their 52,000 known Omicron cases and 17,000 known Delta cases between Nov. 30 and Jan. 1. Omicron patients were hospitalized 0.5% of the time, compared to 1.3% of the time for Delta. Of those hospitalized, the median length of stay was 1.5 days, compared to 4.9 days for patients with Delta. Strikingly, not one of the 52,000 patients with Omicron required mechanical ventilation, compared to 11 of the 17,000 patients with Delta. There was 1 death out of the 52,000 Omicron cases (0.002%). There were 14 deaths out of the 17,000 Delta cases (0.082%). Age, comorbidities, and vaccine status were not reported for ventilated patients or deaths. That the single Omicron death was not mechanically ventilated implies that the patient had some reason to elect a do-not-attempt-resuscitation (DNAR) status or died of some sudden cause rather than progressive respiratory failure. Similar reports that describe outcomes in a thoroughly sequenced cohort of Omicron patients are needed (please send them to me when if you see them), and from different settings where vaccination status and other characteristics differ (in this study 49.8% of the Delta patients were unvaccinated and 26.5% of the Omicron patients were unvaccinated).
One-way masking:
Back to the topic of masking, and a term that has recently blossomed in the press: one-way masking. One-way masking means you can choose to wear a reliable mask that, alongside your vaccinations, is so protective against covid (and presumably most/all other respiratory viruses) that it doesn’t matter if others around you are unmasked. From a Jan. 10 Atlantic article on the topic: “If you are vaccinated, boosted, and wearing a well-fitted N95 or similar indoors, “your risk is extremely low,” says Joseph Allen, a COVID and ventilation expert at Harvard. “I mean, there’s not much else in life that would have as low a risk as that. I would qualify your risk as de minimis.” Ever since the CDC recently overhauled the level of detail in their mask guidelines, it has quickly become an excellent go-to source of information for people trying to discuss mask selection and mask fitting objectively. The guidelines make the distinction between a mask versus a respirator, list respirators that meet particular international standards, and even link to a website and webinar to help inform your purchase of an internationally-sourced respirator.
When the time comes that indoor mask mandates get lifted in our state, these clearer sources of knowledge about effective one-way masking strategies can be welcomed reassurance for people who remain at high risk of severe outcomes after infection with SARS-CoV-2 or other respiratory viruses, as well as low risk people who choose masking to help continue their streak of not getting infected with SARS-CoV-2.
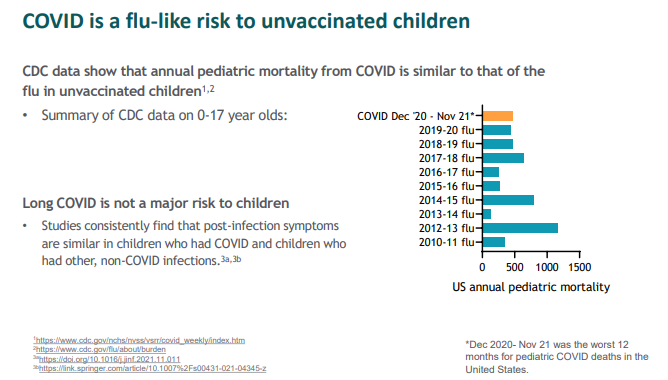
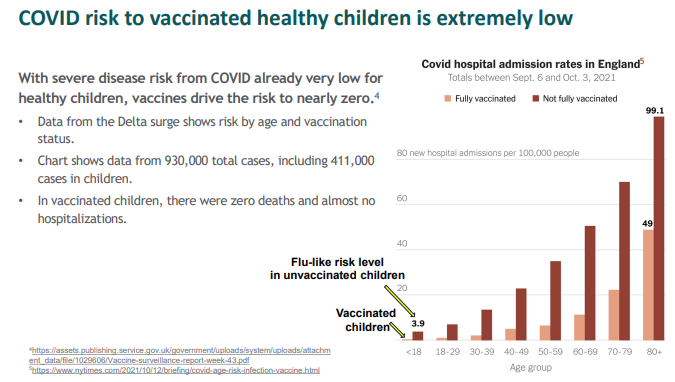
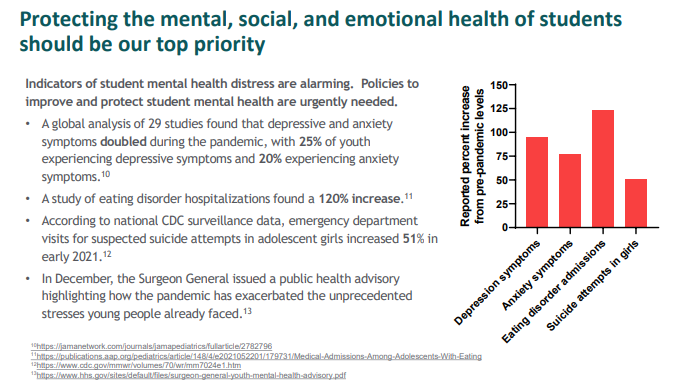
I don’t see any value in someone like me predicting when mask mandates will fall in Washington, but it is my strong personal hope that they fall first in schools. There seems to be a growing conversation about studies and expert reviews like this one citing the difficulties children have understanding speech and identifying facial expressions and emotions when people are wearing masks. Subjectively, in my family, the positive feelings of mental health that washed over me as I witnessed those initial maskless indoor playdates we allowed our two boys (age 5 and 8) after they were vaccinated were so strong they almost brought me to tears. The European equivalent of the CDC doesn’t recommend masks for children under age 12. Here in the US, the position to ease mask mandates for kids is becoming more organized. The Urgency of Normal is an advocacy group of physicians (especially pediatricians) and scientists. Over 850 medical and health professionals (including me) have co-signed their recently published statement of steps needed to restore children’s schools, athletics, and activities to their 2019 norms. That includes making masks optional in US schools by a suggested date of Feb. 15th. Here are some pastes from their online informational toolkit:
Plog on,
Sam
Plogging:
Plogging is a term invented by Erik Ahlström referring to the act of picking up trash and litter while jogging. It is a portmanteau of the Swedish term plocka upp, which means “to pick up,” and jogging.
