
January 5, 2022
Happy 2022 Wise Patient Community,
“Hello friends! How’s your pandemic?” opened the holiday letter from a friend, at once affirming the pandemic has touched each of us but differently. For those of you close to one or some of the 825,000 covid deaths in the U.S. (5.44 million in the world), or someone with a scary hospitalization or prolonged symptoms, the answer surely begins with “Awful” and it would be understandable if the net-optimism I (Sam) hope to build out in this newsletter doesn’t do much to scratch that awful.
For the few of you who haven’t had your heads buried in the pile of covid news stories (I’m jealous of you, by the way), our latest chapter of the pandemic is the Omicron variant spreading quickly around the globe.
Omicron is mind-blowingly infectious:
Case counts of covid exploded in South Africa within the initial weeks following the first scientific description of Omicron that S. Africa readily shared with the rest of the world. Outside of S. Africa, early anecdotes of Omicron superspreading events (remember the restaurant office party in Oslo) have given way to soaring covid case records reported by country after country (reference: headline after headline after headline). The U.S. on Monday reached a record-breaking 1 million documented daily covid cases, with Omicron accounting for 95.4% of samples genetically sequenced as of Jan 1, up from 58.6% as of Dec 25. At UW virology lab, similarly, as of today, ~90% of samples sequenced are Omicron. On an academic side note, not all covid detected can be genetically sequenced for variant type, owing to cost and time constraints. For example, during November, Washington, one of the best-in-class states for sequencing covid samples, sequenced 11.5% of all samples and with great help from the UW virology lab. Beyond the documented covid cases that are shattering records is an unknowable number of uncounted (home test positive, unreported) and undiagnosed cases (symptomatic and not tested, or asymptomatic and not tested) that most of us predict is plenty high. Check out Boston’s wastewater!
Remember, Delta had already been the most infectious variant to date, and aerosolized transmission of it had been well documented on several occasions like this one, better summarized on twitter. Omicron appears multiple times more infectious than Delta. Determining what that exact multiple is is challenged by the denominator problems of sky-high cases not matched by sky-high testing availability. One commonly referenced study, though, from Japan (not yet peer reviewed) using S. Africa data inferred Omicron to be 4.2x as infectious as Delta. Chris Murray, Director of the Institute for Health Metrics and Evaluation (IHME) here at UW, recently forecasted that 60% of the U.S. will get infected with the Omicron variant within the upcoming 2-3 months (peaking late January at about 2.8 million new daily infections before trending down again, with up to 90% of Omicron cases asymptomatic or low symptomatic).
How is Omicron so infectious?:
Spike protein mutations: From the moment the Omicron alarm was sounded in S. Africa, the focus was on the exceptionally high number mutations in the genetic code for the spike protein that allows the SARS-CoV-2 virus entry into the human cells and is the primary target of the approved covid vaccines’ induced immune response. Fortunately, the covid vaccines remain highly effective at preventing severe covid, including from infection with the Omicron variant. Yet, because of the spike protein mutations they are far less effective at preventing any infection with Omicron. More vaccinated people will be infected with Omicron than with prior variants. Even though vaccinated people are less capable of spreading their (breakthrough) cases of covid than unvaccinated people, most infected people with Omicron are still capable of spreading.
Rapid replication in the human bronchus: A Hong Kong research group, using human lung tissue removed for treatment of the lung, normally discarded, observed (not yet peer-reviewed) that the Omicron variant replicates itself 70x faster than the Delta variant and original SARS-CoV-2 in the bronchus, which is a larger air passage closer to your coughing mouth than the smallest more fragile air passages deeper into the lung. In that deeper lung, where oxygen uptake and pneumonia happen, Omicron was observed to replicate much slower than the Delta variant and 10x slower than the original SARS-CoV-2. It is quite plausible that such rapid replication in the bronchus would translate to higher contagiousness with coughing, talking, and breathing. Similarly, it is quite plausible that such a lower replication rate deeper into the lung where pneumonia happens would translate to less severe illness. That brings us to the next topic.
The Omicron-is-less-virulent-
The vast majority of experts have agreed on ‘yes,’ but still debate the degree to which Omicron is less virulent in different age groups and vaccination status groups. First off, the tremendous value of vaccination to protect against covid hospitalization and death has thus far remained as true for Omicron as it did for prior variants. Here in King County, in the 30 days ending 12/22/2021, people not fully vaccinated were 33x more likely to be hospitalized for covid and 45x more likely to die from covid than those fully vaccinated. All the news I read from S. Africa, the UK, New York, and other locations with well-documented Omicron waves seems in agreement that those dramatic relative differences in outcomes between vaccinated groups and unvaccinated groups will likely continue over time, even if/when hospitalizations and deaths fall after Omicron peaks similar to how they fell in S. Africa. The covid vaccines that we have (correction: that we rich countries have much more of) continue to work well!
Using the S. African Omicron data to reassure ourselves in the U.S. has been met with some criticism. Since I am plagued by optimism, I have been doing so anyway. After all, S. Africa has a lower vaccination rate, lower booster rate, and an eye-popping HIV prevalence of over 20% (really, look it up). Here are two graphs that tell important stories from S. Africa:
.
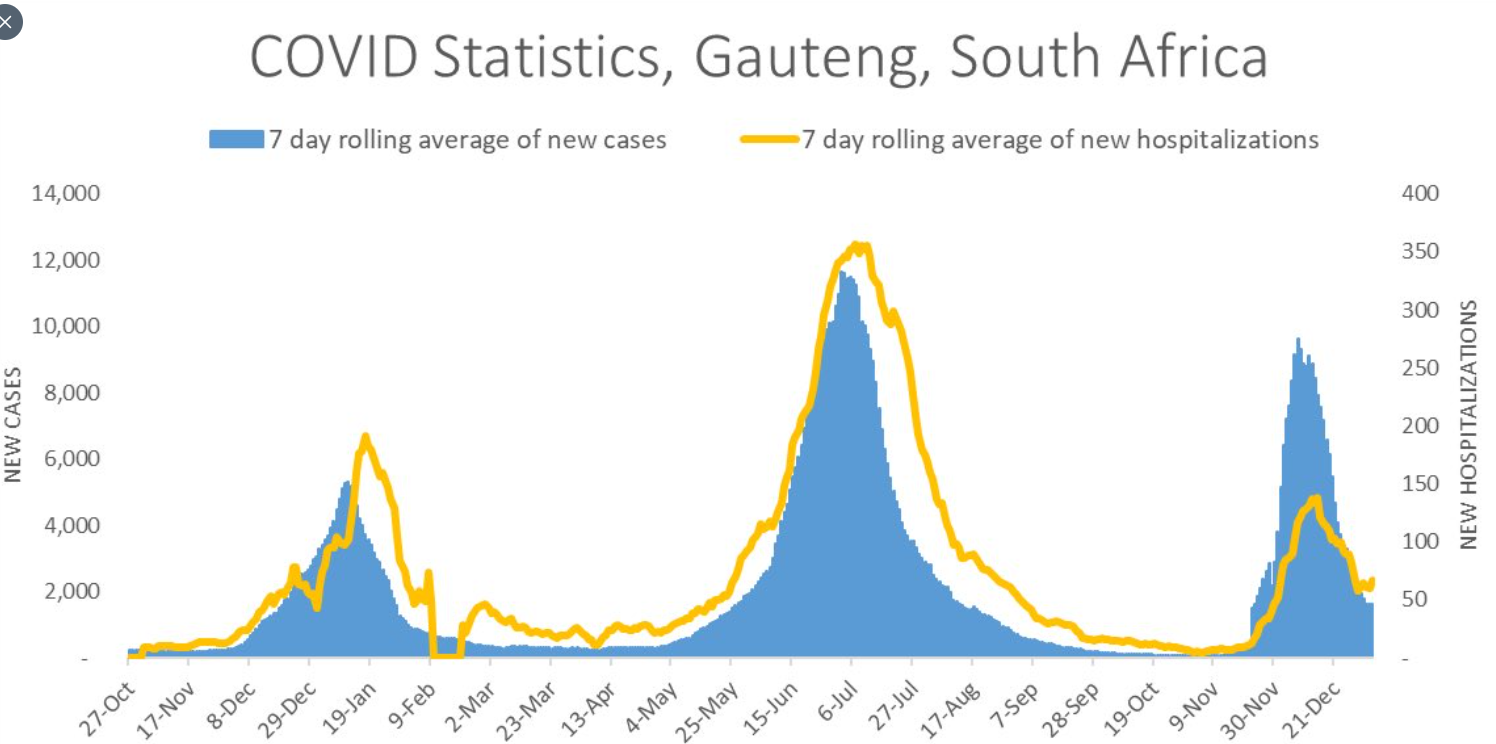
source: South Africa’s National Institute for Communicable Diseases
.
Associated Twitter summary of the above graph from Scott Gottlieb, former FDA Commissioner 2017-2019:
“Revisiting hard hit Gauteng region of South Africa, where Omicron wave first visibly emerged, cases continue to fall sharply, hospitalizations remained decoupled from prior waves and also fall. The entire epidemic wave lasted about two months, and took one month to reach its peak.”
And look below at how low the up-to-date Covid death rate in S. Africa with this Omicron wave is compared to past waves. We are beyond the time point when such a comparatively low death rate could be explained away by lag time between covid illness and covid death, especially when hospitalizations are decidedly declining in the Gauteng region.
.

.
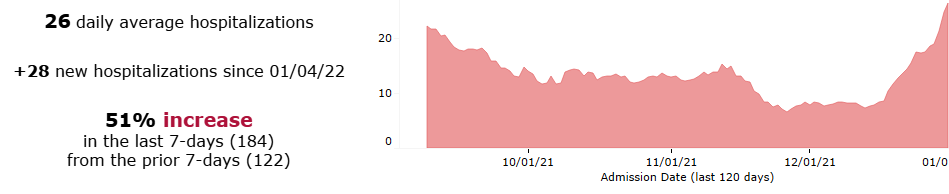
Getting selfish, I tried to zero-in on Seattle and San Francisco right now with those cities’ best-in-country level of covid vaccination. Unfortunately, it seems we need more time before we breathe our collective sigh of relief (that I, plagued by optimism, believe will come:). Hospitalizations are still increasing. From King County’s covid dashboard:
.
.
Our local increase in hospitalizations is the more concerning amid anecdotes of a decreasing number of healthcare workers able to work due to home isolation and quarantine.
.
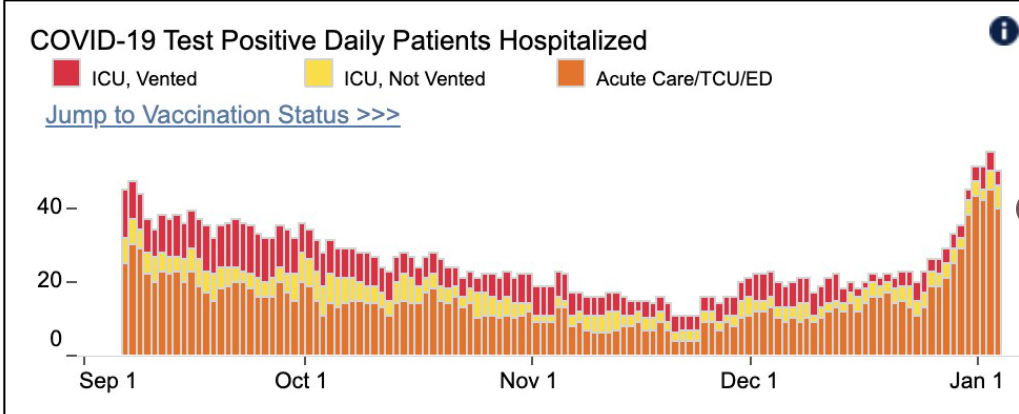
For San Francisco, I looked at this graph posted by Bob Wachter (2 days ago), Professor and Chair of the Department of Medicine at the University of California, San Francisco (UCSF):
.
.
… and his associated tweet of cautious optimism: “Patient #’s @UCSFHospitals stable at ~50 x 4d – w/ ICU % low.STILL TOO SOON TO BE SURE(!) &, to me, an argument to be MORE CAREFUL, but it’s hopeful. Omicron may be hitting a big immunity wall in SF.”
New calendar years for me are about new wishes:
My realistic wishes for covid in Q1 2022 (I’m plagued by optimism, remember) are:
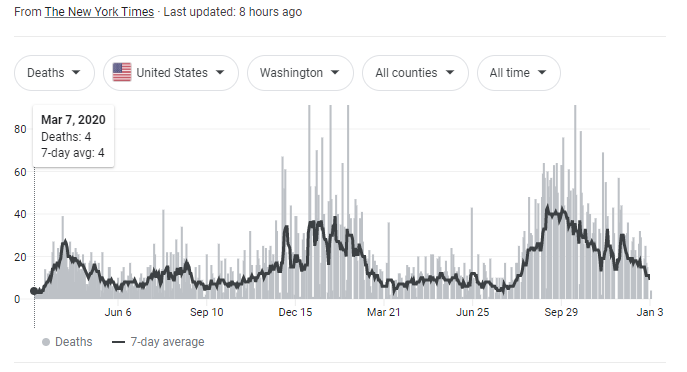
1) The covid death rate in Washington continues to decline despite the massive Omicron wave, and drops sharply once Omicron infection (expectedly but not yet proven) provides increased protection against the more deadly Delta variant – especially important for unvaccinated people. New antiviral therapeutics become available for people at highest risk of severe covid, including severely immunocompromised people who mount poor immune responses to vaccines and past infections.
.
.
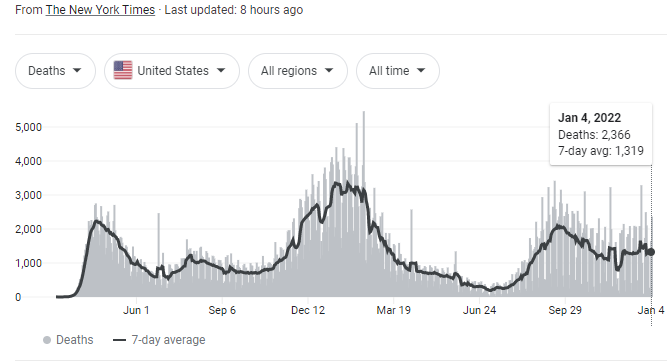
2) The covid death rate in the US, pretty flat since October-ish, drops sharply through a similar rationale.
.
.
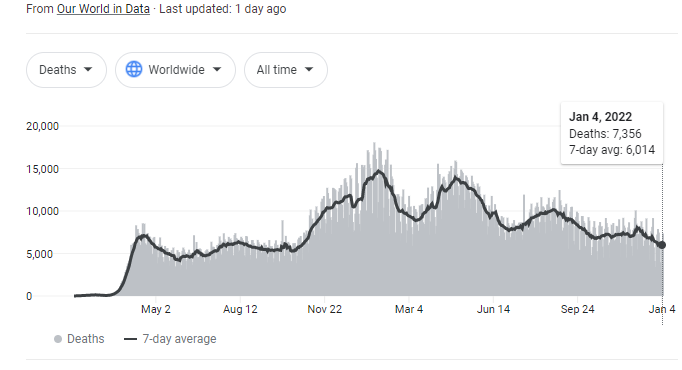
3) The covid death rate worldwide drops sharply through a similar rationale, despite the embarrassing differences in access to vaccines and upcoming embarrassing differences in access to new antiviral therapeutics.
.
.
My realistic longer-term wish for covid in 2022 and beyond (lest you forget I choose optimism, a well-vaccinated form of optimism) is that this Omicron wave is the beginning of the end of the pandemic. That Omicron plus vaccines completely outcompete the Delta variant. That the resulting wall of immunity is strong enough and long-lasting enough, including against more new variants that are likely to keep coming, to progress the world into a clearly endemic SARS-CoV-2 virus. Through vaccines, periodic re-infection (similar to with the 4 types of coronavirus that have caused common colds for some time), and a range of treatment options to prevent high risk people from dying, SARS-CoV-2 gets relegated to a much inferior rank of threatening pathogens. Over time, with collective effort, may the many social tolls of the pandemic, for example this one, be reversed.
Sam
PS: I was going to write some about the upcoming oral antivirals Paxlovid and molnupiravir, as well as about the randomized clinical trial from Brazil on fluvoxamine, an SSRI mood medication repurposed to treat outpatient covid, but ran out of time. Suffice it to say, if you test positive for covid and you are a patient of ours, let us know and we will do our best to personalize a strategy for you.